
Replantation
Amputation injuries are devasting injuries where parts of the limbs are severed, either completely or incompletely. Amputations can involve the whole limb (termed major amputations) or just the fingers (termed digital or minor amputations).
Major amputations involve the limb at the wrist, forearm, elbow or upper arm levels. They are termed major as they can be life-threatening, and the amputated part contains a lot of muscles, making it not being able to survive more than 4-6 hours without blood flow. Muscles tolerate ischemia (lack of oxygen) poorly, and this period of ischemia can be prolonged by cooling the amputated part.
After stabilising the patient’s condition, major amputations need to be operated on immediately to reconnect the blood circulation to the severed part as quickly as possible. Establishment of circulation is first achieved with a shunt (tube) connecting from the artery of the stump to the artery of the amputated part. Formal replantation (re-attachment) involves debridement (removal of dead or contaminated tissues), bone shortening and fixation, repair of tendons and muscles, and reconnection of the nerves and blood vessels under microscopic magnification, The skin is then closed, or covered with skin graft or flap.
|
|
|
| Right arm amputation injury through the elbow after reattachment. | |


Digital (or minor) amputations involve the fingers or thumbs, which do not have muscle tissues and hence can tolerate the loss of blood circulation longer, although it should still be done within 4-6 hours. Surgery is similar to major replantation surgery, except that there is no need to establish an immediate shunt circulation. After debridement, bone shortening and fixation, and repair of tendons, microsurgical repair of nerves and blood vessels is done with the microscope up to 20 times magnification for vessels down to 1mm in diameter or smaller. This makes digital replantation surgery technically challenging.
First aid to the amputation injury patient at the site of injury include cleansing and bandaging of the wound to stop bleeding, and cooling the amputated part by putting it in a plastic bag and then putting the bag into another plastic bag containing ice and water. This helps the tissues to survive a longer period without blood circulation.
The suitability and success of replantation surgery depends on the medical fitness of the patient, type of injury, duration of time the injury had occurred, level of amputation, and age of the patient.
|
|
|
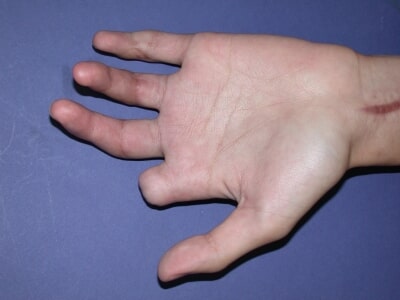
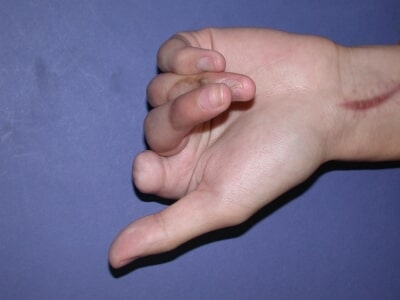
| Avulsion amputation of left thumb replanted with good result | |


Sharp injuries are better than crush or avulsion injuries (where the limb or digit is pulled out). An example of an avulsion injury is ring avulsion injury, where the finger is pulled off when the ring is caught by a fixed object. The faster the circulation is established, the better. The smaller the part (i.e., further from the body), the better. Younger patients also recover faster and better, probably because of the ability of the nerves to regenerate better.
|
|
| Grinder injuries are devastating involving multiple levels. |

|
|
|
|
|
| Grinder injury with successful replantation of 3 fingers with fair function. | |||


Not all amputations can be replanted. Lower limb amputations are often not replantable, as the function is generally not good, and prosthesis can function better. However, parts of the leg or foot can sometimes be used to cover the stump to preserve length for better function with the artificial limb.
For the hand, reconstruction of the lost thumb or finger can be done with toe-to-hand transfers, where either the big or second toe is used to fashion a thumb or finger, using microsurgical techniques. Other techniques can also be done to improve hand function, such as lengthening the stump. Arm and finger prostheses are available for improvement of appearance and function.
|
|
|
| Amputated thumb reconstructed with big toe. | |

