
Nailbed and Fingertip Injuries
Nailbed and fingertip injuries are common as we use our hands for everyday activities. The nail provides protection for the fingertip and allows us to pick up small objects as it provides a counterforce to the finger pulp during pinching. Nailbed injuries are common in children (accounting for two-thirds hand injuries in children) and blue collar workers.
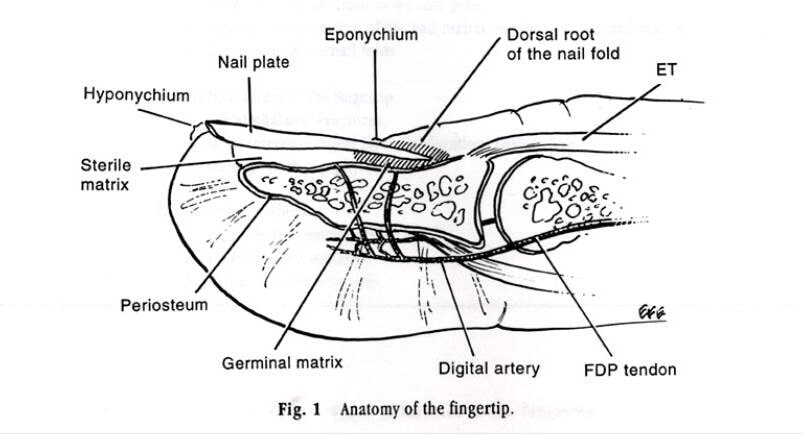
The nail complex comprises of 3 parts
- Nail-plate – Hard structure composed of keratinized squamous cells
- Sterile and Germinal matrix –nailbed below the nail-plate that is supported by the underlying distal phalanx .The Germinal matrix produces 90% of the nail-plate while the more distal sterile matrix provides close adherence for the growing nail-plate.
- Dorsal and lateral nailfolds- defines the boundaries of the nail-plate, adds shine to the nail-plate.
Most injuries of the nailbed involve the fingertip as a result of crush injury by doors or machinery. There is often a laceration of the nailbed with a disrupted nailplate. It could also involve a fracture of the underlying bone if the forces are great. The importance of care for these patients is that a proper debridement of the open wounds are performed surgically so that wound infection is prevented, followed by an accurate repair of the nailbed so that the new nail that grows subsequently will be normal.
When this is neglected, granulation tissue forms under the nail plate and it becomes very difficult to accurately oppose the nailbed subsequently. It will result in nailbed scarring and as scar tissue isunable to produce nail material, this will lead to characteristic defects during regrowth of the posttraumatic nail. It can cause a split or absent nail, or a nonadherent nailplate.
|
|
|
|


